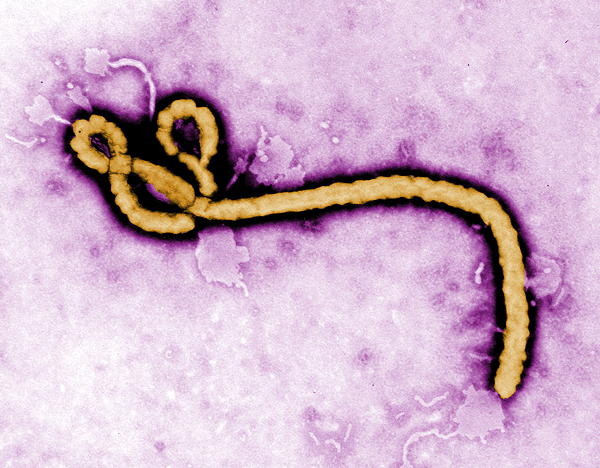
In 1976, Fred Murphy, a virologist working at the CDC, saw the long, filamentous Ebola virus for the first time under electron microscopy and took the artificially colored image on this page. He was also the only expert that had looked at the Marburg virus, a close cousin to Ebola.
Ebola hemorrhagic fever has become know as Ebola Virus Disease, or EVD. Initially a rare disease, it has repeated on even ongoing epidemics in Africa. Various strains of the virus have now been seen around the globe.
It is spread through contact with either an infected wild animal or another person. There is variability of mortality, and in the case of the Reston Ebolavirus, known as RESTV, even symptoms it exhibits. Ebolavirus has an extremely efficient ability to be absorded into living cells, where it replicates explosively. The virus reproduces so quickly that it overwhelms the host immune response. Before antibodies can be produced against the spike proteins that attach to, and cause absorption by, the target cell, widespread cellular infection occurs in all tissues, other than bone.
The initial infection appears to come through wild infected animals which harbor the virus without being harmed by it. In Africa, a staple of the diet in areas where Ebola has been seen seem to begin with consumption of “bush meat” from these animals. The local or rural form gives way to the urban form.
Once infected, the virus spread from person to person. All body fluids team with Ebola. While the incubation period last for up to twenty-one days, the first symptom of fever and headache appears around nine days or so. Historically, death from widespread hemorrhage occurs often by around twelve to fourteen days.
There are different strains of Ebola which exhibit different mortality rates. Ebola Zaire, was named for the Ebola River near the village of Yambuku in what is today known as the Democratic Republic of Congo. The word “Ebola” means black, and the acronym EBOV refers to the Ebola Zaire strain. The mortality rate for Ebola Zaire. Ebola Sudan, in retrospect, was probably the first on the scene in southern Sudan which is near Yambuku. It is designated by the acronym SUDV. EBOV and SUDV have mortality rates typically in the 90% and 50% range, and these two account for the majority of Ebola cases in the world. Mortality rates seems to be affected by the speed of diagnosis and implimentation of intensive supportive care and fluids. This is not a given though, as many notable and well-trained African physicians and other health care workers died after caring for Ebola patients. The overall mortality among Ebola strains is around 50%.
The Ebolavirus strain discovered in Reston, Virginia and Alice, Texas at the Hazelton monkey facilities wreak havoc among monkeys, but cause few, in any symptoms, among humans. The book The Hot Zone and the National Geographic series by the same title together tell a chilling history of Ebola in the US. It is known by the acronym RESTV, and it originated from a monkey farm in the Philippines which sold the animals to the Hazelton company.
The Taï Forest strain, known as TAFV, was isolated in Parc National de Taï, in Côte d’Ivoire. The single known case of TAFV was contracted by a forest researcher who survived the illness.
The Ebola Bombali strain, known as BOMV, was found in Angolan free-tailed bats in Taita Hills, Kenya. Infection in humans was not found in my research.
The chain of infection seems clear though the index animal source of Ebola has yet to be confirmed. Infection brews in wild animals which are consumed by local populations. Person to person spread is quick and efficient through body contact which is especially enhanced with the twenty-one day asymptomatic incubation period. Prodromal symptoms include fever, muscle aches and pain, fatigue, sore throat, and headache, and can easily be deemed a “case of the flu.” Vomiting and diarrhea ensue and become bloody and a hemorrhagic skin rash appears. Bleeding progresses both internally in all organs, and externally from all body orifices. Mucous membrane linings of the gut are sloughed off and expulsed with the diarrhea, and other mucous membranes in the stomach, etc., slough off as well. Liver enzymes skyrocket as vast numbers of hepatic cells rupture and liquefy. Hemorrhage affects the brain and a morbid, blank stare ensues. The kidneys fail as the virus kills renal cells. Severe pain and agony precedes death from multiple organ and circulatory failure. All body fluids teem with billions upon billions of infectious Ebola virus particles.
Cultural practices vary by locale, and have been problematic in Africa where touching and kissing deceased persons at funerals occur. The virus remains viable on the body for a substantial period after death, and the contagion is so easy that even with the strictest of biological barrier protections there is a risk.
Diagnosis
Diagnostic testing can be confirmed with these possible methods. All samples should be handled with level 4 biohazard precautions.
- antibody-capture enzyme-linked immunosorbent assay (ELISA)
- antigen-capture detection tests
- serum neutralization test
- reverse transcriptase polymerase chain reaction (RT-PCR) assay
- electron microscopy
- virus isolation by cell culture.
Treatment
Antiviral treatments so far have not been terribly effective. Intravenous fluids and blood transfusions are important, but once the gut begins to slough its mucosal membrane, these treatments become futile. There are some drug trials you can read about here. Blood from recovered patients has been used in the African field as a last effort to save patients. The monoclonal antibodies Inmazeb and Ebanga are approved by the US Food and Drug Administration.
Vaccines
There are two vaccines that show particular promise, though supplies are probably limited because of the high manufacturing cost compared to the ability to cover research expenses. Ervebo was approved in December 2020 by the US Food and Drug Administration. The WHO prequalified its use for Ebola Zaire, EBOV, in those 18 and older who are not pregnant or nursing. In the 2018-2020 Ebola outbreak in the Congo it was given under compassionate using it to “ring” a wall of immune individuals around outbreak areas.
The second vaccine is a really a combination of the Ervebo vaccine given first followed 8 weeks later by a subsequent dose of the newer Mvabea vaccine. This combination can be given to those 1 year and older, but because of the long time frame between doses, is not useful in epidemic outbreaks.
Considerations for Survivors
Recovery from Ebola virus does not mean all is necessarily well. Ebola can persist in semen, testicular tissue, eyeball fluids, breast milk, and pregnancy related fluids. Relapse is not common, but not unknown either, and the reasons for it are not understood. The PCR, or polymerase chain reaction, can be persistent positive for even up to nine months after recovery from acute disease. The reasons are not know, but I must point out that PCR testing is a screening test and cannot be used as a definitive diagnostic.
![]() Copyright secured by Digiprove © 2021 Ronnie Smith
Copyright secured by Digiprove © 2021 Ronnie Smith
 Copyright secured by Digiprove © 2021 Ronnie Smith
Copyright secured by Digiprove © 2021 Ronnie Smith
Recent Comments